Medical Treatment
Cervicobrachial disorders, low back pain, knee pain

Dr. Grip ballpoint pen, which became a worldwide hit.
My specialty is occupational health, and I have been working as a corporate occupational physician for more than 30 years. At Yuwa Clinic, we have an outpatient clinic specializing in occupational diseases. Please consult with us anytime.
New meridian therapy is very good at treating pain and is extremely effective for these common painful conditions that are often seen at work or on a daily basis.
Stress on the cervicobrachial, lumbar and knee muscles causes muscle fatigue, which gradually leads to the accumulation of lactic acid and other fatiguing substances. When this becomes chronic, intense pain occurs. If the pain persists for a long time (often more than three months), it is stored in the spinal cord and becomes intractable. It is recommended that patients receive treatment as early as possible before the pain is stored in the spinal cord.
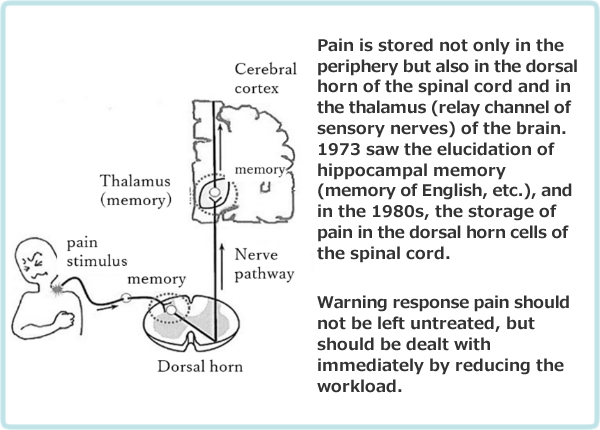
Figure 1-2. Memory of pain
Cervicobrachial Disorder(referred to as CBD)
CBD is a disorder that causes symptoms such as fatigue-related pain, numbness, and coldness in the cervicobrachial region caused by prolonged, repetitive use or holding the upper limbs up, such as when using a computer. Progressive pain in the upper limbs makes it difficult to work.
In addition to personal computers, other types of work such as telephone exchange, supermarket checkout, childcare, meal preparation, assembly of electrical products, and sign language interpretation have also been associated with this disorder.
Work Control Standards for Keypunchers
In 1957, key punchers at Nippon Telegraph and Telephone Public Corporation (now NTT) had an outbreak of cervicobrachial disorders. NTT was one of the first companies, along with banks and securities firms, to introduce computers.
Computers at the time were based on punch cards, which were inserted into a machine with holes in them, which were then read to input data and perform calculations. The key puncher's job was to punch holes in the cards by pressing keys on the punching machine. Three to four keystrokes per second were required, with tens of thousands to 100,000 touch heavy keystrokes per day.
Keypunchers and typists were the flowery occupations of the time, and many young women yearned to be employed. In this glamorous occupation, a cervicobrachial disorder developed.
Doctors at the time were surprised that a light task such as keypunching could cause severe cervicobrachial disorders. Some researchers then began to study cervicobrachial disorders. Even when I was an industrial physician at Nisshin Steel in the 1970s, more than 20 key punchers were working, and I was conducting medical examinations for cervicobrachial disorders.
Later, in 1962, the onset of the disease in a key puncher at N Securities Company made the headlines and attracted social attention as an occupational disease.
This incident led to the notification of a Labor Ministry directive on work management for keypunchers in 1964. Until then, it was normal for keypunchers to work for eight hours a day, but to prevent CBD, keypunching should be limited to 300 minutes a day, or five hours a day, with a continuous working time of 60 minutes, 10 to 15 minute breaks in between, and 40,000 touches per day or less.
This was a landmark notice, as it was the first time that a daily work time limit and a single continuous work period were enforced. This was the model that later led to work hour regulations for cash registers and sign language.
Later, CBD also developed in the assembly of electrical products and in the manufacturing of cigarettes and other products. At this time, many conveyor-based flow operations were widespread, and the increased density of work was the cause of the onset of the disease.
In 1973, a notice was issued to prevent CBD due to working as a cashier in a supermarket, which led to the establishment of the Yuwa Clinic.
Subsequently, the disorder expanded beyond the previous clerical work to include childcare workers and school lunch cooks. All of these occupations were complicated by back pain.
In 1984, CBD and eye strain have become major problems in VDT work, and guidelines have been issued. In 1990, the issue of CBD in sign language interpreters was addressed.
Example of Treatment of Cervicobrachial Disorder(CBD)
The following is a case study of new meridian therapy of CBD of a sign language interpreter. This case illustrates the effectiveness of the therapy in the treatment of chronic and severe CBDs.
- A. Chief complaint
- pain and numbness in neck, shoulder, and arm
- B. Abstract
- The patient had worked as a sign language interpreter for 30 hours a week for 11 years and suffered from severe CBD including neck, shoulder, and arm pain, numbness, hand tremor, insomnia, and difficulty in housework. The patient has been suffering from chronic and severe CBD for 11 years. In general, when CBD becomes chronic and severe (Japanese Society for Occupational Health, CBD Severity Level IV or higher), the disease becomes intractable. This case is also diagnosed as a Grade IV, refractory condition.
- C. Current medical history
- After working for an interpreter, she interprets for up to 7-8 hours a day. On days when there are many visitors, she interprets for about eight people. She was so busy that she could not even take a lunch break.Later, she became aware of cervicobrachial pain and tremor in her hands. She had difficulty doing housework and trouble sleeping due to the pain, but her sense of duty kept her going.
At the time of the survey, she was interpreting an average of 3.7 people a day. (The National Association for the Study of Sign Language Interpreting Problems proposed a standard of 2 interpreters per day.)
After treatment at a nearby bone-setter clinic, she was instructed to reduce the amount of interpreting work, but continued to do so without taking time off from work.
After a medical checkup for sign language interpreters, she was diagnosed with CBD IV and applied for leave of absence from work and workers' compensation. - D. Course of Treatment
- Physical examination reveals pain, dull pain, and numbness in almost all areas of the neck and arms: the nuchal muscle (posterior neck), trapezius (shoulder), supraspinatus, levator scapulae (scapula), and anterior scalene muscles (anterior neck). New meridian therapy is used for these symptoms. After 3 months of treatment (total of 12 treatments), she returned to work after her symptoms improved. She works as a sign language coordinator on a full-time basis. Progress is good with monthly follow-up.
- E. Conclusion
- As described above, the new meridian therapy has been shown to be remarkably effective in cases where aftereffects remain. In our case, the remarkable efficiency was observed in 80% to 90% of chronic and severe cases, and we believe that it is effective as a central therapy for cervicobrachial disorders.
Preventive measures for computers
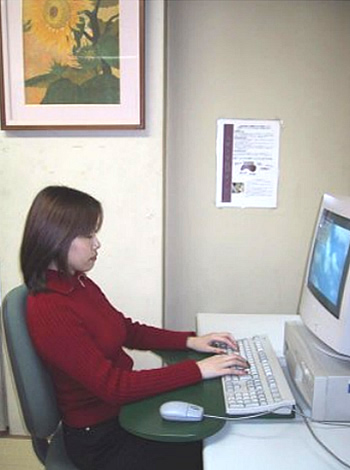
Fig. 1-4 illustrates the armrest we have developed in use. The figure shows a good working posture with the back resting firmly against the vertical backrest, the head not tilted forward, the arms not in the air, and the forearms resting on the armrests, keeping the eyes away from the computer screen.
Armrest is a device to which the user “rests” their “arms”. The armrest can be adjusted by fastening it to the desk with Velcro tape, and the keyboard is placed on it. The mouse can then be used on the wide right side of the board. This armrest is placed between the user and keyboard which enables the left and right arms to rest on it. The stomach area is concave, so that the user can position himself close to the desk. This protrusion is very important. This shape reduces the burden on the neck and shoulders when working on a computer.
Low back pain
Low back pain is the second most common ailment after the common cold, and it is estimated that about 80% of adults will experience low back pain at least once in their lifetime. The main causes of back pain are muscular back pain and herniated discs.
Low back pain from heavy handling
It is well known that lifting and carrying heavy objects is a major cause of low back pain. In Japan, based on a person's weight, 40% of his body weight is used as the standard for a male. In other words, for a person weighing 60 kg, the weight should be regulated to 24 kg or less. For women, the standard is 60% of a man's weight; a woman weighing 50 kg should be regulated to no more than 12 kg.
Back pain in bad posture
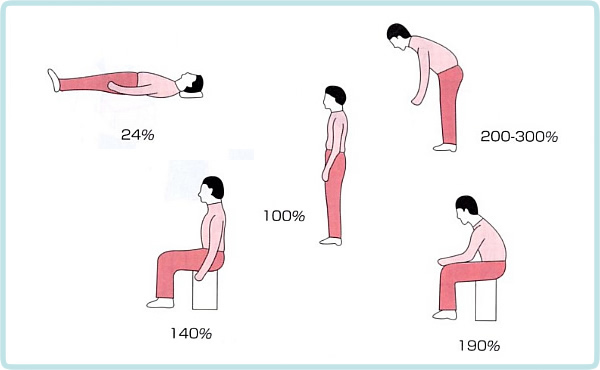
Fig. 1-4 shows an index of the load on the lumbar spine by inserting a needle into the intervertebral disc between vertebrae 3 and 4 and measuring the internal pressure of the disc. With the standing position as the reference (100%), the lumbar burden of the other four postures is expressed numerically.
The five postures have a higher lumbar load in this order: supine < standing < sitting < forward bending. Standing is the posture with the least lumbar strain. The walking posture is more desirable.
The forward bending posture, in particular, is two to three times more stressful than the standing posture. This is due to the strain on the lower back to support the weight of one's own upper body even without having to carry heavy objects. For this reason, the forward-bending posture, along with heavy lifting, is a cause of muscle-fatigue back pain.
For this reason, forward bending postures should be avoided by improving the height of the work surface.
Low back pain from prolonged sitting
In recent years, computer work has become widespread, and an increasing number of people sit and work on computers for long hours throughout the day. As a result, back pain caused by prolonged sitting has been increasing.
The mechanism by which prolonged sitting causes low back pain is shown in Fig. 1-6.
1)Sedentary posture causes the pelvis to tilt backwards, and causing the physiological lordosis of the lumbar spine to disappear. To correct this, the muscles in the low back are strained, causing muscular back pain.
2) Due to the loss of physiological anterior curvature, strong pressure is exerted on the front of the intervertebral disc. The pressure exerted on the closed space by Pascal's principle acts to increase the pressure on the entire disc reducing the flow of spinal fluid, which supplies nutrition, in and out of the disc. This inhibits the regeneration of the fiber ring due to malnutrition, resulting in the deterioration progresses.
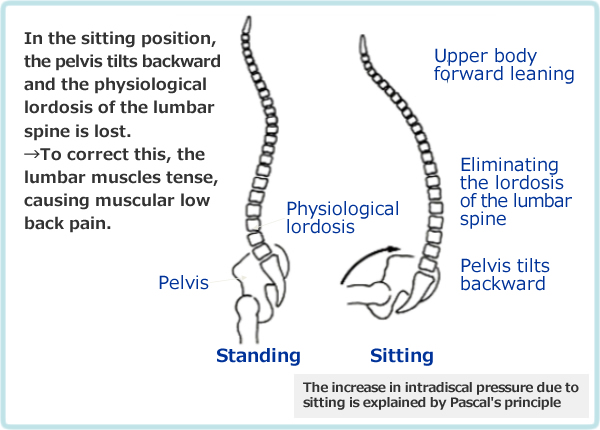
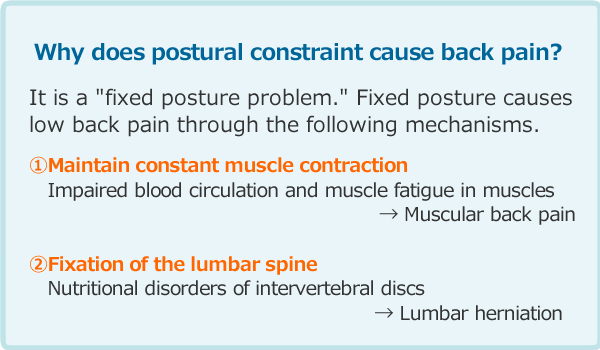
Figure 1-7 illustrates how a fixed seated posture can cause low back pain. In any good posture, a fixed posture without motion causes deterioration of the intervertebral discs due to a decreased supply of nourishing spinal fluid. Deterioration then weakens the intervertebral disc, and the slightest impact can cause the fiber ring of the disc to fail and the nucleus pulposus to eject, resulting in a lumbar herniation.
Example of treatment for lumbar hernia
32-year-old male, lumbar hernia between lumbar vertebrae 4 and 5.
- Chief complaint
- left buttock pain, dull pain.
- He developed lumbago when lifting a 30 kg sugar bag at work in the morning. He is wearing a corset.(See Fig.1-15) He complained of pain and dull pain in the left hip. Examination reveals a hernia between lumbar 4 and 5.
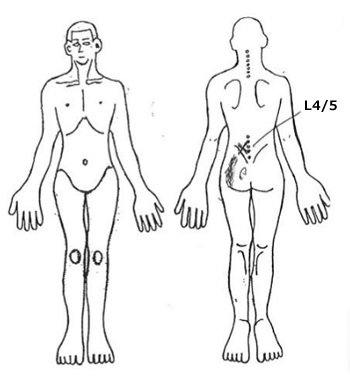
Figure 1-7. left L4/5 tapping pain, and pain & dull pain in the hip 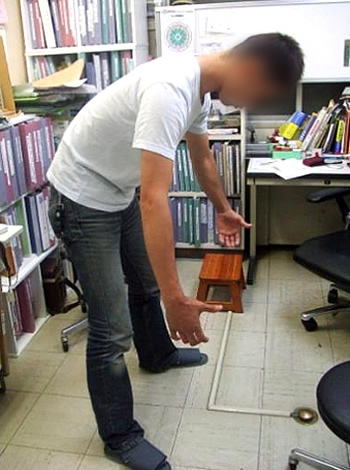
Figure 1-8: Sugar bag lifting posture in forward bending - Progress
- Pain in the low back and hip improved after 3 sessions of new meridian therapy. The progress is good. As you can see, it depends on the symptoms, but it improves quickly.
- Guidance
- Lifting weights in a forward-bent posture is very stressful on the lower back and can cause low back pain. To avoid this, the patient was instructed to bend the knees, avoid forward bending of the low back, and use knee strength to lift.
Another way to reduce the burden on the low back is to use a pelvic belt, as shown in Fig. 1-9. The belt increases abdominal pressure and makes the abdominal cavity as tight as a rugby ball, relieving up to 30% of the upper body burden into the abdominal cavity and reducing low back strain. (Fig. 1-10) For repetitive lifting of heavy objects, use a powered lifting balancer as shown in Figure 1-11.
Figure 1-9: Pelvic belt reduces the low back burden 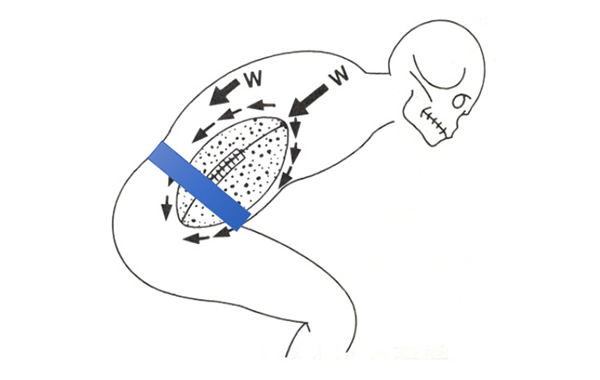
Figure 1-10: Mechanism of the belt's effectiveness in reducing lumbar strain
Rugby ball theory of increasing abdominal pressure
Figure 1-11: Lifting and moving a 20 kg paint can with a balancer.
The can is adsorbed by negative-pressure air, lifted by power, and moved without weight.
Knee arthritis
Most patients develop symptoms such as knee pain, movement disorders, and joint edema as a result of workload such as prolonged standing, handling heavy objects, work that involves rotation of the knee in a flexed position, obesity, and bowleg. It often develops gradually after middle age and is accompanied by internal/external deformity, quadriceps atrophy, limited range of motion, tenderness in the joint fissure, and joint edema.
New meridian therapy is also effective in difficult cases with deformities. For treatment, if obesity is present, new meridian therapy is performed simultaneously with weight loss through carbohydrate restriction.
Treatment case of knee arthropathy
60-year-old woman with lumbar spondylolisthesis and right knee arthropathy
She has had knee pain for 5 years. She has been treated at the hospital but without any effect. When she pushes a wheelchair to take care of her family, she begins to feel the knee pain strongly. She is obese, with a height of 155 cm and a weight of 59.4 kg. She has tried more than 10 different diets, but all have failed. She is trying to lose weight by restricting her carbohydrate intake while undergoing new meridian therapy.- Progress of treatment
- After 6 Tx of new meridian therapy, the patient was able to go down the stairs with ease. 13 Tx of therapy, the patient forgot about the pain in her knee. After 16 Tx, the patient was cured completely.
Table 1-2 shows the progress of the carbohydrate-restricted diet. In the first 10 weeks after the start of the diet, her weight and body fat percentage decreased by 8.6 kg and 8.9%, respectively. There has been no rebound since then, and the patient is very surprised. This case is an example of chronic knee arthritis associated with obesity without bone or joint bone deformity. The carbohydrate-restricted diet contributes to the improvement of knee pain symptoms and the prevention of recurrence, and is extremely effective when used in combination with the new meridian therapy.Table 1-2. Progress of weight loss by carbohydrate restriction Elapsed days Body weight (kg) Body fat (%) Initial visit 59.4 33.6 14days 56.9 30.7 28days 54.7 29.0 42days 53.3 25.5 56days 52.7 26.4 70days 50.8 24.7