Medical Treatment
Postherpetic neuralgia
Postherpetic neuralgia is a nerve pain that causes pain memory in the spinal cord and brain as well as nerve pain in the chest and abdomen and the limbs. This pain memory is stored in the spinal cord in as little as 3 weeks after the onset of shingles, when the pain persists. And the more time that passes, the stronger the pain memory becomes and the harder it is to heal.
Therefore, the appropriate treatment for postherpetic neuralgia is new meridian therapy, which is effective not only in treating nerve pain in the peripheral regions, but also in treating nerve pain in the spinal cord and brain.
Postherpetic neuralgia is one of the most intractable nerve pains. There is no effective treatment for it in Western medicine. As a result, many people suffer with pain.
First treatment case
The first treatment case is a man in his 70s. His daughter, who had known about our clinic's treatment, contacted us because her father was suffering from shingles pain and she was eager to have him treated. The pain was seen from the left side back to the chest and abdomen. He visited a dermatologist because of a rash in March 2008. The rash improved after taking antiviral medication, but the pain did not go away, so he visited an anesthesiologist who diagnosed him with postherpetic neuralgia in the left thoracic region and he was hospitalized for 3 weeks.
The treatment relieved some of the pain, but the hospital told him to be prepared for aftereffects because he could not sleep because of the pain.
In June of the same year, he visited our hospital. Three months had already passed since the rash, and the condition had progressed to intractable postherpetic neuralgia. He had a scar on his left abdomen from the shingles, continued insomnia due to tightening pain in his abdomen, and still had severe pain in his left back.
After two new meridian therapies, the pain was slightly relieved, after six treatments the back pain was further relieved, and after seven treatments the abdominal pain improved.
The pain was so severe that he was unable to watch TV, but after 9 treatments, the pain was reduced by half and he was able to watch TV and said he felt like going on a trip. 25 treatments were completed with almost no pain.
Thus, the new meridian therapy is a pain-relieving treatment for patients suffering from postherpetic neuralgia. Since then, we have treated many patients with postherpetic neuralgia, and their intractable neuralgia improves promptly.
I will first describe other treatment cases and then discuss the mechanism of postherpetic neuralgia.
Other treatment cases
Treatment case 2.
postherpetic neuralgia after angina pectoris
- Chief complaint
- Left-sided chest pain
- Medical History
- In December, he was admitted to a general hospital for angina pectoris. After discharge from the hospital, on December 28, he developed pain and a rash on the left side of his chest. Due to the year-end holiday, he visited the hospital one week later on January 5, and was diagnosed with shingles and given antiviral medication. The rash has improved, but the chest pain has persisted for the next two years without relief. He is currently undergoing treatment at a neurosurgery unit and is taking Tegretol (used for antiepileptic drug and pain relief). Initial pain rating (VAS) was 10/10, but now VAS 3-4/10 remains. Tingling and tingling pain continues.
- Previous medical history
- 2005- Repeatedly in and out of hospital with angina pectoris, with multiple cardiac stents in place.
Onset Factors: Herpes zoster due to lowered immunity after angina pectoris surgery and delayed initial treatment due to year-end holidays, presumed to have induced neuralgia. - Time from onset to new meridian treatment
- 2 years and 3 months

Figure 4-2. Postherpetic neuralgia in the left thoracic region 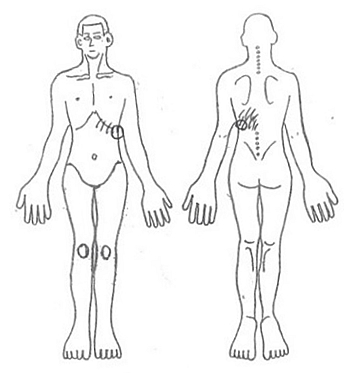
Figure 4-3. Painful areas - Progress of treatment
-
- Just after 1st Tx
- tingling becomes a little lighter.
- After first Tx
- 2 days after the treatment, he feels better. However, after 7 hours of weeding and other yard work, he became ill.
- 8 Tx
- the progress is good.
- 9 Tx
- the pain decreased.
- 10 Tx
- VAS improved to 2/10. After 15 treatments, he stopped covering his chest with his left arm.
- 15 Tx
- Shingles pain is not bothersome at times. It is only painful sometimes.
- 17 Tx
- VAS is less than 1/10, and the patient is cured.
- Summary
- A case of postherpetic neuralgia due to delayed initial treatment. After the onset of the disease, the pain did not go away for 2 years and 3 months. This is a case of abbreviated cure after 17 sessions of new meridian therapy.
Treatment Case 3.
Postherpetic neuralgia in the shoulder associated with diabetes mellitus
- Chief complaint
- Electroshock pain in the shoulder 3-5 times every 10 minutes
- Medical History
- Diabetic for 3 years and on medical treatment (HbA1c 6.2). In March of this year, he took care of his two grandchildren. In late April, he developed pain in his left shoulder and a rash. He took an antiviral drug, Amenalief , but the pain persisted, so she visited a pain clinic on May 6.
Pregabalin (Lyrica) 75 mg 2T(2) and Tramcet combination tablets 8T(4) (maximum dose) are taken for 2 months from May 6 to July 4, but with limited effect and no further improvement.
Taste: alcohol: 1 can of beer and 2 go(about 360cc) of liquor. Exercise habits: 1.5 hours of daily walking.
- Previous medical history
- Diabetic for 3 years. 2 years ago, cataract surgery on right eye.
- Factors in the onset of the disease
- Shingles is presumed to have been triggered by a lowered immune system due to diabetes and fatigue from taking care of grandchildren, etc.
- Time from onset to new meridian therapy
- 2.5 months
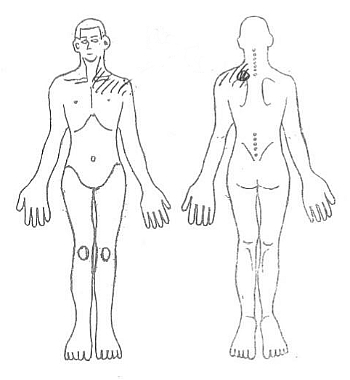
Figure 4-4. Painful areas 
Figure 4-5. Comparison of shingles skin rash on the chest and shoulders before and after new meridian therapy. The skin rash has disappeared with treatment. - Progress of treatment
-
- Just after 1st Tx
- Shoulder pain reduced.
- After 1st Tx
- deep shoulder pain is reduced. No more rubbing on the painful part of the shoulder. Tingling electric shock pain 3-5 times in 10 minutes.
- 2 Tx
- the electric shock pain is reduced to once every 30 minutes.
- 3 Tx
- he did farm work in the morning. He was less concerned about the pain.
- 5 Tx
- pain score improved from VAS 5/10 to 2/10.
- 9 Tx
- VAS reduced to 1~2/10.
- 14 Tx
- the region of pain became narrower.
- 15 Tx
- VAS reduced to 1/10 or less. Before the visit to the clinic, Tramcet was 4T per day, but after the visit, the dosage was reduced to 2T per day.
- 16 Tx
- VAS becomes 0.5/10.
- 17 Tx
- HbA1C improved to 5.8 with carbohydrate restriction and postherpetic neuralgia became generally healed.
- Summary
- This is an example of treatment of post-herpetic neuralgia in the shoulder caused by diabetes and fatigue. Improvement was achieved by new meridian therapy combined with carbohydrate restriction. It shows that carbohydrate restriction is important to improve immunity.
Treatment Case 4.
Case of facial paralysis due to Hunt's syndrome
46-year-old woman
- Chief complaint
- Left facial nerve palsy, spaghetti overflowing from the corner of the left mouth, left eyelid not closing (rabbit eye), forehead not wrinkling.
- Medical History
- In March of this year, the patient was admitted to the Otolaryngology Department of the University Hospital with a diagnosis of Hunt's syndrome. The patient presented with a skin rash on the left auricle to the head and was treated with antiviral drugs and systemic steroids. There is no hearing loss or vertigo. On discharge from the hospital, her facial nerve palsy score was 9/40, indicating complete paralysis, with 40/40 indicating normal. In April of the same year, new meridian therapy was administered.
- Cause of Onset
- Worked late into the night as a PC instructor at a newly established company and was overworked. She also had many opportunities to drink alcoholic beverages.
- Time from onset to new meridian therapy
- 1.2 months later.

Figure 4-6. Mouth distortion improved after 21 new meridian treatments. - Treatment course
-
- After 4 Tx
- facial nerve palsy score improved to 13/40.
- 13 Tx
- the patient's mouth lifted better.
- 19 to 20 Tx
- the score improved to 32/40.
- 21 Tx
- the distortion of the corners of the mouth improved.
- 22 Tx
- the score improved to 36/40 (improved to 90%)
- 23 Tx
- the score improved to 38/40 (Normal)
- Summary
- The score of facial nerve palsy after drug treatment was 9/40, which was considered a case of complete paralysis, but the patient was cured without paralysis with 38/40 after new meridian therapy. The results showed that the new meridian therapy was effective in treating facial nerve palsy such as Hunt's syndrome. (Courtesy of Dr. Keiko Hiragun)
Postherpetic Neuralgia Pain
Figure 4-7 shows the mechanism to postherpetic neuralgia. Prolonged herpes zoster pain causes postherpetic neuralgia in about 20% of people. The pain is then stored in the peripheral nerves, trigeminal nerve, dorsal horn of the spinal cord, and thalamus of the brain. The dorsal horn of the spinal cord is a cluster of nerve cells at the back of the spinal cord where the sensory nerves enter. It is called the dorsal horn of the spinal cord because it is sharp like a horn.
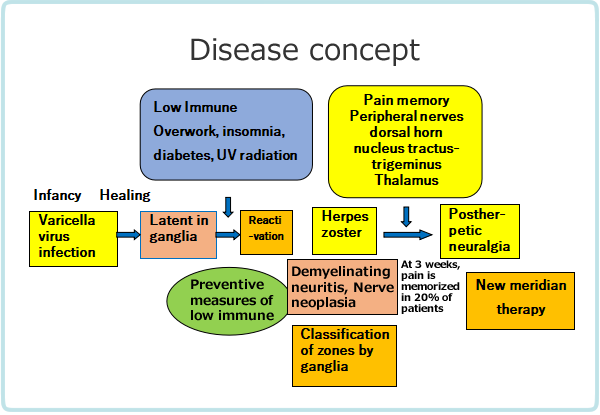
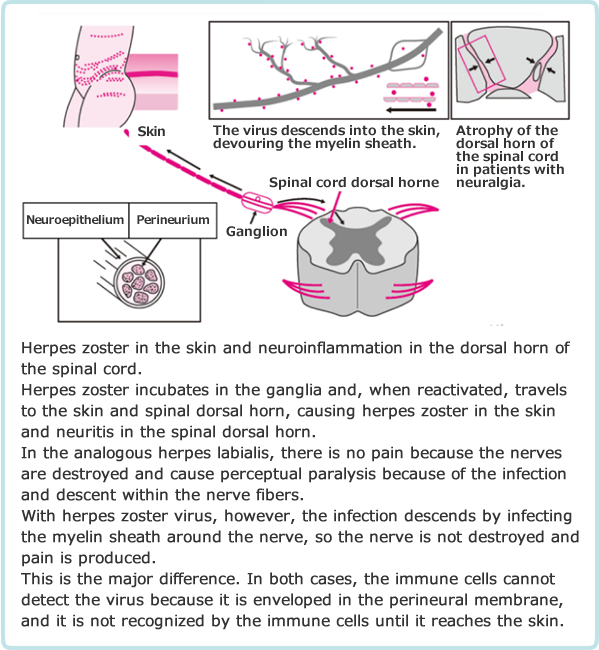
Figure 4-8 illustrates the mechanism that causes neuralgia. Viruses that multiply in the ganglia descend to the skin and cause shingles, while at the same time ascending the nerves to reach the dorsal horn of the spinal cord and cause infection, resulting in inflammation of the dorsal horn of the spinal cord, and neurotrophic factors secreted by small glial cells (repair cells) that gather to repair the inflammation, causing nerve regeneration, hyperalgesia (feeling pain more intensely than usual), and allodynia (feeling pain when touched).
Postherpetic neuralgia is a condition in which the nerve itself spontaneously combusts, causing pain. It is very painful, and in some humans, there are cases of electric shock pain that recurs for a day, once every 20-30 seconds. The pain may include tingling, visceral tightness, and burning pain.
This persistence of postherpetic neuralgia pain is due to pain memory from long-term excitation of the nerve junction (called long-term potentiation), combined with proliferation of painful nerve circuits following inflammation of the spinal cord dorsal horn by the virus.
Pain Memory.
After 3-4 weeks of shingles, when the pain does not subside, the acute phase of shingles shifts to post-herpetic neuralgia. The mechanism of the transition is that the pain is stored in the dorsal horn of the spinal cord. Once the pain is stored, it becomes resistant to treatment and becomes more intractable the longer it has been present. There is a wide range of theories on this transition period, ranging from two weeks to three months, but I use a transition period of at least three weeks to ensure that the transition to neuralgia is minimized.
Treatment effectiveness depends on the time since onset of illness.
The "ease/difficulty of healing" of shingles is strongly influenced by the time since onset of shingles.
Dr. Masayoshi Hyodo, Professor of Pain Clinic, Department of Anesthesiology, Osaka Medical College (at the time of the paper), stated, "When pain is still present more than one month after the onset of illness, it is called post-herpetic neuralgia (PHN). Especially when more than three months have passed since the onset of the disease, nerve block therapy no longer yields good results. In particular, nerve block therapy is hopelessly ineffective in patients who have had the disease for more than one year.”
Dr. Bunkichi Wakasugi, founder of the Japanese Pain Clinic and professor emeritus of anesthesiology at the Jikei University School of Medicine in Tokyo, states that "the shorter the time from herpes zoster onset to the start of treatment, the better the prognosis, with 6 months being the boundary of this time frame (see Table 4-1). That is, within two weeks of herpes zoster onset, the complete/generally healing rate is 90%, whereas for cases beyond six months, the generally healing rate drops sharply to 10%." Wakasugi's data shows that even within one to six months, the generally healing rate drops to 27.6%.
Thus, if left untreated, the memory of pain becomes stronger and more intractable, so early treatment is necessary.
| Within 2 weeks | 91.2% |
| Within 1 month | 63.1% |
| Within 6 months | 27.6% |
| Within one year | 10.1% |
| Within 3 years | 15.5% |
| Within 5 years | 15.1% |
| Over 5 years | 11.1% |
Treatment Outcome of New Meridian Therapy for Postherpetic Neuralgia
Out of 50 patients presenting with herpes zoster or post-herpetic neuralgia and treated with new meridian therapy, 46 patients with complete VAS data on pain related to herpes zoster at the initial and final visit and data on treatment course were analyzed for treatment outcome. The average age of the patients was 58.2 years and 63.1 years for women.
| Disease type | Total | Postherpetic neuralgia | Acute-phase shingles |
|---|---|---|---|
| n | 46 | 34 | 12 |
| Hunt’s syndrome | 4(8.7) | 4(11.8) | 0(-) |
| Trigeminal nerve | 4(8.7) | 4(11.8) | 0(-) |
| Occipital nerve | 4(8.7) | 4(11.8) | 0(-) |
| Thoracic/upper back | 9(19.6) | 8(23.5) | 1(8.3) |
| Upper abdomen/middle back | 18(39.1) | 13(38.2) | 5(41.7) |
| Lower abdomen/low back | 14(30.4) | 10(29.4) | 4(33.3) |
| Lower back/lower limb | 16(34.8) | 8(23.5) | 8(66.7)※ |
| Whole body | 1(2.2) | 1(2.9) | 0(-) |
p<0.05, Significance accepted. (X-square test Yates' correction)
Table 4-2 shows the types of herpes zoster according to the classification of Hiroyasu Ishikawa et al. All patients with Hunt’s syndrome, trigeminal and occipital nerves had postherpetic neuralgia, suggesting that these types are more likely to have sequelae. Herpes zoster in the thoracic/upper back and face tended to be particularly refractory and prone to sequelae.
The factors of pathogenesis estimated from the interviews are as follows. For postherpetic neuralgia, 50% for fatigue, 23.5% for insomnia, 23.5% for abdominal surgery/peritonitis, and 20.6% for immunosuppressants such as steroids. Fatigue and insomnia are the biggest causes of weakening the immune system. Abdominal surgery also lowers immunity due to the burden of surgery. Immunosuppressive drugs for atopy and rheumatism were also major factors.
Recently, there have been an increasing number of cases of postherpetic neuralgia due to a weakened immune system related to the new coronavirus. First of all, it is essential to be careful not to overwork yourself.
| Outcome | Total(%) | Postherpetic neuralgia | Acute-phase shingles |
|---|---|---|---|
| n | 46 | 34 | 12 |
| Greatly improved | 34(73.9) | 22(64.7) | 12(100) |
| Moderately improved | 10(21.7) | 10(29.4) | 0( - ) |
| Slightly improved | 1(2.2) | 1(2.9) | 0(-) |
| No change | 1(2.2) | 1(2.9) | 0(-) |
| Worsening | 0( - ) | 0( - ) | 0( - ) |
Table 4-3 shows the effectiveness of the new meridian therapy. In acute-phase shingles, the improvement rate was a very high 100%. For acute-phase shingles, Dr. Keiko Hiragun, a dermatologist, reported that almost 100% of patients with 330 cases of acute-phase shingles were able to avoid the transition to postherpetic neuralgia by combining antiviral drugs with new meridian therapy.
New meridian therapy is extremely effective for shingles in the acute phase, and when combined with antiviral drugs, the patient recovers quickly. Previous reports indicate that approximately 20% of people with acute-phase shingles will transition to neuralgia. With the new meridian therapy, this can be avoided. This is a very significant effect.
The effect on postherpetic neuralgia was shown to be as high as 94.1%, including a significant improvement of 64.7% and a moderate improvement of 29.4%, while most reports indicate an efficiency of about 20% for conventional treatment. New meridian therapy is an effective treatment for postherpetic neuralgia.
Table 4-4 shows the effectiveness of the new meridian therapy when the time from onset to treatment is classified as less than 2 months, 2 to 6 months and more than 6 months in the most difficult-to-treat category.
The most difficult-to-treat patients, who had been treated for more than six months, showed a 46.2% marked efficacy and 46.2% effective, with a combined efficacy rate of 92.4%, which is a high and satisfactory rate.
In conventional treatment, the generally healing rate is said to fall sharply to 10% after six months after the onset of shingles, and the results of the present treatment greatly exceed this.
| Time since onset | Total | Greatly improved | Moderately improved | Slightly Improved | No change |
|---|---|---|---|---|---|
| Total | 46 | 34(73.9) | 10(21.7) | 1(2.2) | 1(2.2) |
| < 2 months | 25 | 22(88.0) | 2(8.0) | 0(-) | 1(4.0) |
| 2- 6 months | 8 | 6(75.0) | 2(25.0) | 0(-) | 0(-) |
| ≧ 6 months | 13 | 6(46.2) | 6(46.2) | 1(7.7) | 0(-) |
Conclusion
The effectiveness of the new meridian therapy for postherpetic neuralgia, even in cases with a long course from the onset of the disease, is effective enough to satisfy patients compared to conventional treatment. It is also an excellent treatment that does not cause any burden to the body and avoids the transition of acute herpes zoster to neuralgia. It is recommended for those suffering from postherpetic neuralgia.